Ebola in Uganda, Tanzania, DRC, Kenya, Rwanda, and Burundi: Regional Risk, Patterns, and Response
Ebola is a viral disease that appears intermittently in parts of Central and East Africa. It does not circulate continuously in the general population, but when it emerges, it can spread quickly through close contact and create serious public health pressure. In the Great Lakes region, countries such as Uganda, Tanzania, the Democratic Republic of Congo (DRC), Kenya, Rwanda, and Burundi remain connected through travel, trade, and shared ecosystems. This connectivity shapes how Ebola risks are monitored and controlled.
The disease does not affect all countries equally. Some have experienced repeated outbreaks, while others mainly prepare for possible spillover cases. Even so, regional coordination is essential because outbreaks do not respect borders.
What Ebola Is and How It Spreads
Ebola is caused by the Ebola virus, which leads to severe illness by damaging the immune system and internal organs. It belongs to a group of infections called viral hemorrhagic fevers.
Transmission happens through direct contact with infected bodily fluids. These include blood, vomit, stool, urine, saliva, and other secretions from a sick person. Infection occurs when these fluids enter the body through the eyes, mouth, nose, or broken skin.
It can also spread through contaminated objects such as bedding, clothing, or medical tools if they are not properly disinfected. In some outbreaks, the virus first enters humans through contact with infected wildlife, especially bats or primates in forested environments.
Ebola does not spread through air, water, or casual interaction. Simple contact like sharing space or walking past someone does not transmit the virus.
Ebola in Uganda
Uganda has experienced several Ebola outbreaks over the years. These outbreaks have occurred in different regions, often near forested areas where human and wildlife interaction is more likely.
The country has developed strong outbreak response systems over time. When a suspected case appears, health teams quickly isolate the patient, begin testing, and start contact tracing. Uganda’s response capacity has improved significantly due to repeated experience managing outbreaks.
Most outbreaks in Uganda have been contained relatively quickly compared to earlier years. This improvement is linked to faster reporting from health facilities, better laboratory systems, and trained rapid response teams operating at district level.
Ebola in the Democratic Republic of Congo (DRC)
The DRC has experienced more Ebola outbreaks than any other country in the region. Many of these outbreaks have been large and complex due to geography, population movement, and sometimes limited access to remote areas.
The virus has often appeared in forested regions, where human activity overlaps with wildlife habitats. Some outbreaks have spread across multiple provinces, requiring large-scale national and international response efforts.
Because of frequent outbreaks, the DRC has become a key center for Ebola research, vaccination campaigns, and treatment innovations. Cross-border coordination with Uganda and Rwanda is especially important due to frequent movement across shared borders.
Ebola in Tanzania
Tanzania has not experienced the same number of confirmed Ebola outbreaks as Uganda or the DRC. However, it remains at risk due to its geographic location and travel connections with affected countries.
In the past, suspected cases have triggered strong surveillance and screening responses, especially when outbreaks occur in neighboring regions. Tanzania focuses heavily on border monitoring, disease surveillance, and preparedness training for health workers.
The main strategy in Tanzania is prevention and early detection rather than outbreak containment, since large confirmed outbreaks have been rare.
Ebola in Kenya
Kenya has never recorded a large-scale Ebola outbreak, but it remains at risk due to its role as a regional travel and trade hub. Airports, road networks, and cross-border trade routes make surveillance a key priority.
Kenya maintains strong screening systems at points of entry, including airports and major border posts. Health authorities are trained to identify symptoms early and isolate suspected cases for testing.
Preparedness programs in Kenya focus on rapid response capacity, laboratory readiness, and public awareness among health workers rather than ongoing outbreak management.
Ebola in Rwanda
Rwanda has not experienced major Ebola outbreaks but remains highly alert due to its proximity to the DRC. Movement across the border is frequent, making surveillance and preparedness essential.
Rwanda has invested in strong health system organization, including training health workers to recognize symptoms early and respond quickly to suspected cases. Border screening measures are also regularly reinforced during outbreaks in neighboring countries.
The country’s strategy emphasizes early detection, strong coordination with regional partners, and rapid isolation of suspected cases.
Ebola in Burundi
Burundi has also not recorded large Ebola outbreaks, but like Rwanda and Tanzania, it remains part of the regional risk zone due to its proximity to the DRC.
Health authorities focus on preparedness, surveillance, and public health education. Border regions are especially important for monitoring because of cross-border movement for trade and family visits.
Burundi’s approach is mainly preventive, with emphasis on reporting systems and coordination with regional health networks.
Symptoms and Disease Progression
Across all these countries, Ebola presents the same pattern of symptoms. It typically begins with sudden fever, fatigue, muscle pain, headache, and weakness. These early signs can resemble malaria or other common infections.
As the disease progresses, vomiting, diarrhea, and abdominal pain may develop. Severe dehydration becomes a major concern. In some cases, bleeding may occur, but it is not present in every patient.
The disease can worsen quickly without treatment. Early medical care significantly improves survival outcomes.
Regional Surveillance and Detection Systems
East African countries use shared surveillance systems to detect outbreaks early. Hospitals and clinics are required to report suspected cases immediately.
Laboratories in the region have improved testing capacity, allowing faster confirmation of cases. Uganda, in particular, has played a central role in supporting regional diagnostic readiness.
Contact tracing teams are activated immediately when a case is suspected or confirmed. These teams monitor all individuals who had close contact with the patient for a defined period.
Treatment and Vaccination Efforts
There is no universal cure for Ebola, but supportive care improves survival. Treatment includes hydration, fever management, and monitoring of organ function.
Vaccines are used during outbreaks, especially for health workers and people exposed to confirmed cases. This targeted vaccination approach helps limit spread.
Countries like Uganda and the DRC have been key locations for vaccine deployment during active outbreaks.
Cross-Border Cooperation in the Region
Because people move frequently between Uganda, DRC, Rwanda, Kenya, Tanzania, and Burundi, Ebola control depends heavily on cooperation between governments.
Countries share surveillance data, coordinate border screening, and support each other during outbreaks. This cooperation helps reduce the risk of cross-border transmission.
Regional organizations and international partners also support training, laboratory work, and emergency response planning.
Public Health Challenges in the Region
One of the main challenges is delayed reporting of symptoms in some areas. Early symptoms can resemble common illnesses, leading to late diagnosis.
Another challenge is misinformation during outbreaks. Rumors can spread quickly and reduce trust in health systems.
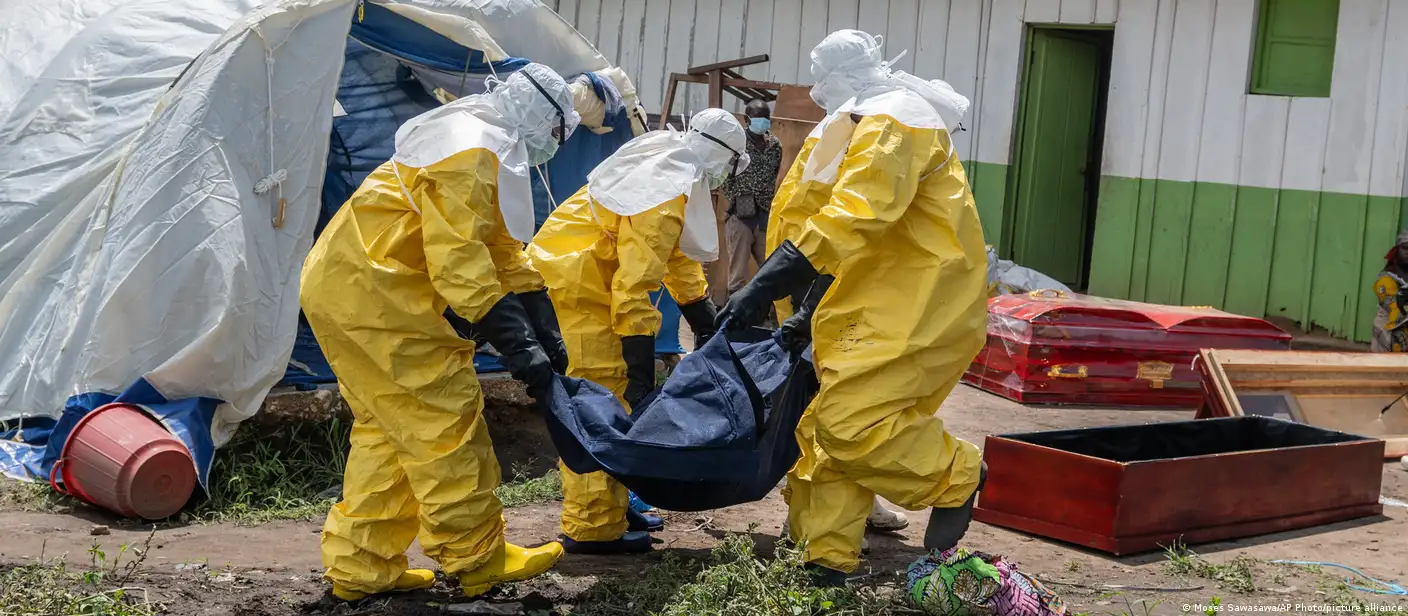
Cultural practices, especially burial traditions involving close contact with the body, also require careful management to prevent transmission.
Impact on Travel and Daily Life
During outbreaks, countries may introduce screening at airports, border posts, and major transport routes. These measures focus on identifying symptomatic travelers rather than stopping movement entirely.
Trade and travel usually continue with monitoring in place, since the region depends heavily on cross-border economic activity.
Tourism is generally not affected unless an outbreak occurs close to major wildlife or travel zones.
Lessons from Regional Experience
The region has learned that early detection and fast response are the most important tools in controlling Ebola. Countries that identify cases quickly are able to limit spread more effectively.
Another key lesson is the importance of coordination. Since borders are porous and travel is frequent, no single country can manage Ebola alone.
Community engagement also plays a major role. When people understand the disease and trust health workers, outbreaks are contained more quickly.
Ebola risk in Uganda, Tanzania, DRC, Kenya, Rwanda, and Burundi varies, but the entire region remains connected through movement and shared ecosystems. Uganda and the DRC have experienced the most outbreaks, while countries like Kenya, Rwanda, Tanzania, and Burundi focus more on preparedness and prevention.
Strong surveillance systems, cross-border cooperation, and rapid response capacity continue to reduce the impact of outbreaks. While Ebola remains a serious threat, regional coordination has significantly improved the ability to detect and contain it before it spreads widely.




{kind=link}